20 February 2015 - Geneva - Country Coordinating Mechanisms (CCMs) are country-level multi-stakeholder partnerships, responsible for coordination and collaboration on Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) related processes in country. Therefore CCMs are important for national ownership and participatory decision-making
According to this first ever analysis on CCM composition by the Stop TB Partnership, based on the data provided by the Global Fund, there is a need for increased TB representation in CCMs in order to reflect the TB situation, and, especially, the needs of communities and key affected populations.
There is a clear under-representation of TB expertise in CCMs, especially in TB High Burden Countries (HBCs). This might eventually result in the lack of proper understanding of TB epidemiology, interventions and prioritization.
According to the Global Fund, CCMs need to be broadly representative of all national stakeholders in the fight against the three diseases. The CCM needs to be as inclusive as possible and seek representation of all key stakeholders that are relevant in the fight against the three diseases in the national context.
In order to ensure vulnerable and marginalized groups are adequately represented, the Global Fund wants the CCMs to find ways to improve the representation and participation of representatives from such groups on the CCM. In addition, the CCM must also reflect the scale of the national epidemics and the key affected populations in the national context with respect to the three diseases.
The Global Fund recommends that all countries strive to include the following actors in their CCMs: Academic/Educational Sector (EDU); Government (GOV); NGOs/Community-Based organizations; People living with HIV/AIDS, TB and/or Malaria (PLWD); Key Affected Populations (KAP); Private Sector (PS); Religious/Faith-Based organizations (FBO); Multilateral and Bilateral Development Partners in-country (ML/BL).
For this report we analyzed data provided by The Global Fund containing the name, gender and role of CCM representatives within the respective CCM, their principal expertise, the constituency and organization they represent. By applying filters to obtain the information of interest and manual counting, we determined the number of representatives with the disease expertise selected, and, within the constituency selected, among the 122 CCMs.
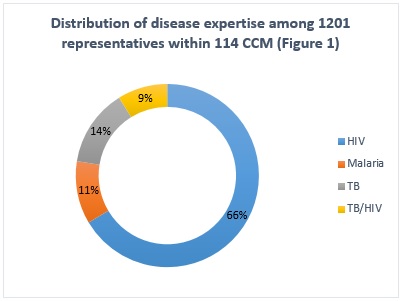
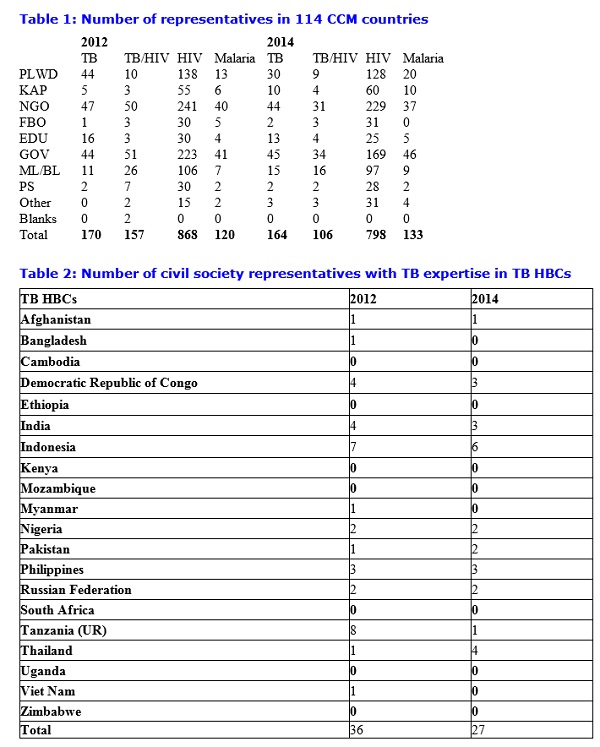
Out of 122 CCMs analyzed, 114 CCMs are recorded with 1201 representatives with disease expertise on either HIV, TB, TB/HIV or Malaria. The number of representatives is not equally distributed among the three diseases and CCMs. Within 114 CCMs, 106 CCMs are recorded with HIV expertise - 798 individuals, only 65 CCMs are recorded with TB expertise - 164 individuals, 50 CCMs are recorded with TB/HIV expertise - 106 individuals and 55 CCMs are recorded with Malaria expertise - 133 individuals (Fig 1, Table 1).
More than that, TB expertise in CCMs is clustered especially in countries that are receptive to engaging TB communities. Getting TB representatives to participate in CCMs remains a challenge in other countries.
The data shows that despite the introduction of joint concept notes for funding, to address the TB/HIV co-infection together, the number of representatives with TB/HIV expertise decreased in 2014 compared to 2012 (Table 1).
The results of the analysis show that in most countries the sectors for People Living With the Disease (PLWD) and Key Affected Populations (KAP) are underrepresented or are absent altogether.
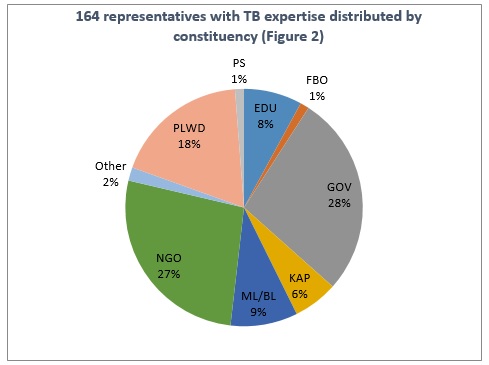
Nearly 60% of the representatives with TB expertise are either from the respective governments or NGOs; people living with TB accounted for 18%, and only 6% belonged to KAP (Fig. 2).
It is one of the core principles of the Global Fund to strengthen the participation of communities and people, particularly those affected by the three diseases. In order to ensure this, the Global Fund�s Guidelines on CCMs (requirement 4) require that all CCMs must show evidence of having at least one member for each of the three diseases (PLWD-HIV, PLWD-TB, PLWD-Malaria) who represents those living with the disease. Additionally, one CCM seat must be filled with a member of KAP. The election of these four CCM seats should be based on epidemiological as well as human rights and gender considerations.
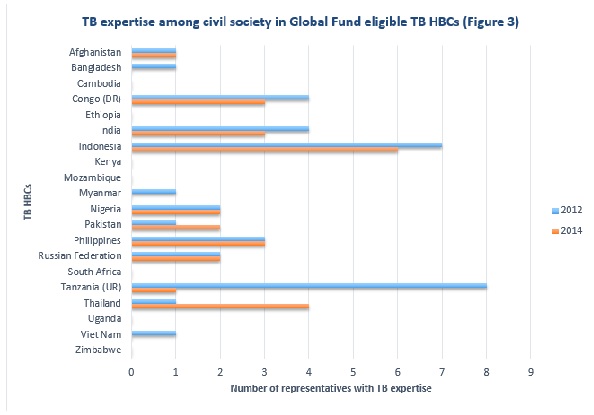
We note with grave concern that half of the TB HBCs eligible for Global Fund grants, have no civil society representative from PLWD, KAP, NGO, FBO or EDU with TB expertise within their CCMs (Fig 3, Table 2). It is even more concerning that, with the exception of Thailand, there seems to be either stagnation or notable decrease of TB expertise from 2012 to 2014.
Further analysis and data is needed to obtain a greater understanding of the level of representation of TB expertise in the CCMs. It will be necessary to coordinate appropriate responses in countries who need to strengthen CCM representation with a particular focus on those who do not have PLDW-TB representation.
The Stop TB Partnership notes these worrying findings and is committed to:
See related story on CCMs that have submitted concept notes are not fully compliant with minimum requirements.
This piece was produced by the Stop TB Partnership led by Lea Rost and Farihah Malik.